Perspectives
Perspectives - June 2025 Edition
CEO BLOG by Keith Bryant
Open Dialogue between Australia and the UKGreetings from the UK, where I am currently visiting as many people and services as I can to create new relationships and a close dialogue between the Open Dialogue Centre in Australia and those who are adopting the approach across services in the UK.
A few days into my arrival, I was fortunate to meet with the Kent and Medway NHS Partnership Trust. They invited me to join day 18 of their 20 day training in Open Dialogue, which was facilitated by Yasmin Ishaq, an Open Dialogue trainer consultant, psychotherapist and clinical supervisor
I also met with teams involved in Central and North West London’s Open Dialogue pilot in Westminster, including the Community Mental Health Hub, Crisis Resolution And Home Treatment team and we discussed Open Dialogue training, early outcomes and the day-to-day realities of embedding the approach in practice. They showed great interest in the work we are doing to shape community-based responses (in the Goulburn Region and Townsville for example) and First Nations experiences of Open Dialogue – around the world. I had a great conversation with Gareth Jarvis who is Medical Director and who interviewed me for his Open POD podcast about Peer Supported Open Dialogue.

Caption: From left to right, Nina Dawson, Sonia Skidmore, Gareth Jarvis, Keith Bryant, Ali Wragg, Liam Hallett, Fiona Eastmond
This was a hugely inspiring visit and I have many insights that I’m excited to share with the team and our partners on my return. The bottom line is that although we are separated geographically, we share similar challenges and aspirations when it comes to implementing change – not just within a service, but in a way that fundamentally changes the mental health system.
On that note, please read my recent article ‘Three ways to support young people with mental ill-health’, published in Pearls and Irritations – an Australian platform for the exchange of ideas, informed analysis and commentary on issues that matter to Australians.
I look forward to the coming weeks where I will be meeting with key people about the ODDESSI results which are due to be published in the next few months. For those who don’t know, ODDESSI is a large randomised control trial, researching the effectiveness of Open Dialogue in crisis and continuing metal health care within the National Health Service in the UK.
Keith Bryant, CEO


‘We are creating the conditions we need to bring the mental health service into the community so that our clinicians are working collaboratively with our community and with peer workers – outside of a clinical environment.’
Sally Thomas, Manager – Infant, Child & Youth Mental Health & Wellbeing Services, Goulburn Valley Health
On June 5th, our collaboration to build a whole-of-community approach to improve youth mental health and wellbeing throughout the Goulburn Region felt alive and energising!
Clear Horizon facilitated a measurement and evaluation workshop on Yorta Yorta Land at the Youth Foyer in Shepparton to support how the Open Dialogue Approach is implemented so that it can be sustained by the community for the long-term.
We had a room full of community partners and young people who participated.

‘A big part of what we are doing is the listening – and then acting on it. For young people who have experienced homelessness, Open Dialogue network meetings present a safe space for dialogue and connection.’
Anita McCurdy, Senior Manager, Shepparton Youth Foyer
As we gain momentum in the Goulburn region, our goal is to identify measures that are meaningful to the community and young people. Embedding their voices in our approach to measurement and evaluation is key to shaping how Open Dialogue will take form across services and as young people live their lives in their community.
What do they need? Where and when? How will we know we have made progress? As the saying goes: Not everything that can be counted counts and not everything that counts can be counted. That’s why getting together to honour the voices of people in the community is so important.
The Open Dialogue Centre is committed to an evidence informed approach. Embedding strong learning and evaluation will help us support our partners and other communities to learn about what it takes to implement community-based responses to mental health, like Open Dialogue.

Exciting news about our One Year Foundation Course!
Tilly Amber Read from Devon in the UK, will co-facilitate block one of our One Year Foundation Course in Open Dialogue, now commencing in Melbourne in September.
Tilly will join ODC’s head of training, Mark Hopfenbeck, to deliver what will be an extraordinary experience for mental health and wellbeing professionals. Together they bring deep expertise around how to implement the approach. Tilly led the implementation of the ODDESSI trial in Devon and she has been instrumental in designing training to support how teams plan, collaborate and foster culture change.
She is a clinical practice lead with extensive experience as a registered mental health nurse. She develops ways to strengthen the understanding of how Open Dialogue can be transformative for organisations and the workforce, with deep knowledge around Peer Supported Open Dialogue, organisational clinical processes, better outcomes for people and families and guidance around developing truly person-centred approaches. Apply now and lead the change in mental health, with strong foundations in improved service delivery backed by the evidence.
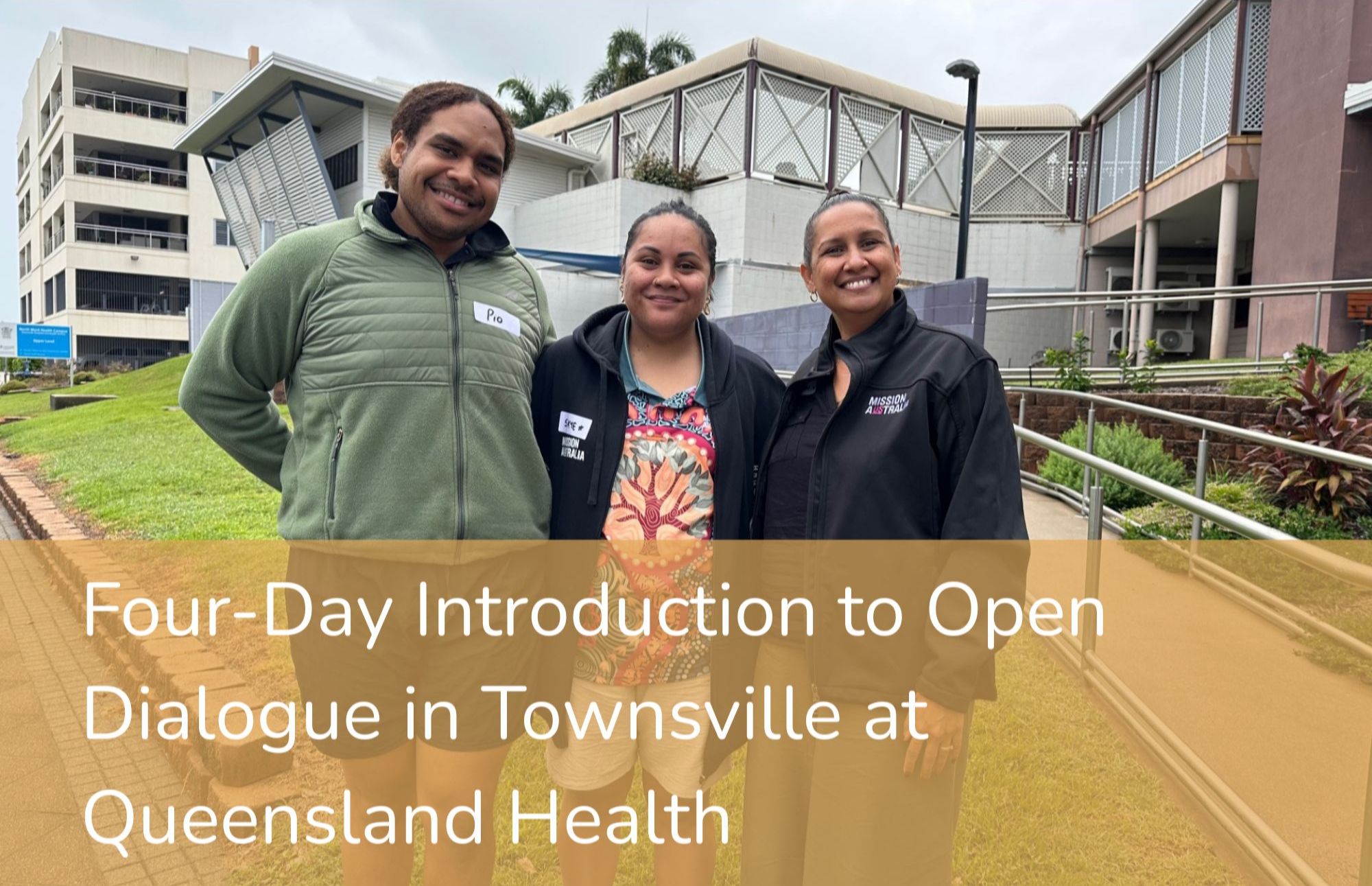
On May 28-29, ODC travelled to Townsville where Mark Hopfenbeck facilitated the second two days of our four-day introduction to Open Dialogue. It was fantastic to see so many people from different local services engaging in conversations and interactive learning experiences about how we can ‘return to something lost’ in the way we approach mental health and wellbeing.
Organisations represented were numerous and included two full teams from Queensland Health including the Early Psychosis team and the Assertive Mobile Youth Outreach team, Mind Australia, One Door, Mission Australia, Townsville Youth Foyer and the Townsville Youth Justice Centre.
In the room we had speech pathologists, care peer support workers, youth development coaches, guidance officers, OT therapists, Lived experience and social workers, psychologists, psychiatrists, managers and coordinators – the full gamut of roles and disciplines involved in community mental health and wellbeing. We extend a big thank you to Elizabeth McNamara and Annette Wilkinson from Queensland Health for hosting and coordinating the four days. We are all looking forward to the next steps.

What can happen when you bring a philanthropist and venture capitalist, Advantaged Thinking and an organisation that is committed to empowering young people together?
Answer: a powerful way to contribute to the growth of the Foyer Foundation and multiply the number of Youth Foyers around Australia!
Founded by John Grant AM in 2009, Grant Family Philanthropy are proud sponsors of the Foyer Advantage Forum in 2025 and foundation partners for the Open Dialogue Centre.

‘I started GFP because I was interested in how collaborative approaches between community services, family and supporters could create environments where young people want to participate – because they feel safe and empowered. We were an earlier supporter of the Foyer Foundation in 2017, and today we are deeply committed to continuing our support for innovative approaches that empower young people and their families to create social networks for mental health and wellbeing in their community,’ says John.
The Foyer Foundation’s invitation to around 200 people to disrupt the cycle of youth homelessness was a huge success on Gadigal Land, Sydney. Among dozens of sessions over several days, Anita McCurdy from the Youth Foyer in Shepparton co-presented with Keith Bryant our CEO and Chair of Foyer Foundation to share the journey so far implementing Open Dialogue within the Berry Street Youth Foyer and beyond in the Goulburn Region.
Save the dates!
Save
the dates!
Upcoming Open Dialogue Programs Enabling services to work towards recovery-oriented care that involves family and community
We are inviting mental health, community health and youth professionals who work in multidisciplinary areas of health and wellbeing to be part of an approach that is transformative and empowering. Open Dialogue programs enable people, families, services and peers to collaborate – enabling the person at the centre to own their recovery journey.
One-Day Online Introduction to Open Dialogue
October 20th, 10am to 3pm
Join us for an informative and inspiring day to deepen your understanding of how the Open Dialogue Approach can be transformative for people, families and the workforce.
Four-Day Online Introduction to Open Dialogue
13th & 14th October 2025
28th & 29th October 2025
9am to 4.30pm
A fantastic way to get a full appreciation of the key principles and elements of Open Dialogue. Participants will learn about:
The origin, history and principles of Open Dialogue
The skills used in network meetings, such as responsive listening and reflection
The key elements of dialogic practice and how to apply them
The importance of self-care and self-work and the need for continual development as a practitioner
The essential and unique contribution of those with lived and living experience and importance of advocating for system change
The concept of a network meeting and the basics of how to initiate and facilitate a network meeting in practice
What the integration of the Open Dialogue approach into your life and work might mean for you.

This training is ideal for mental health professionals, clinicians, community healthcare workers, peer support specialists, general practitoners, and anyone interested in collaborative, network-oriented approaches to mental health.
The primary learning outcome of the One-Year Foundation Course is to support trainees to ensure confidence and competence in facilitating Open Dialogue network meetings.
Block One – 29 September to 3 October 2025
Block Two – 24 to 28 November 2025
Block Three – 16 to 20 February 2026
Block Four – 11-15 May 2026